


Medical-grade wearables are generating more patient data than ever before. The challenge for most healthcare institutions isn’t accessing that data—it’s turning it into consistent, defensible revenue. Claim denials, documentation gaps, and EHR interoperability issues are quietly eroding reimbursement potential for programs that should be thriving financially.
This post breaks down the strategic billing opportunities available through Remote Physiologic Monitoring (RPM), the CPT codes that unlock reimbursement, and the role of AI-powered tools like FinanceCore AI in reducing denials and improving compliance with CMS requirements. Whether your organization is just beginning to scale its RPM program or looking to tighten up an existing one, the frameworks outlined here are designed to help you capture every dollar you’ve earned.
The Evolution of Wearables: From Fitness Trackers to FDA-Approved Clinical Tools
The story of wearable health technology didn’t start in the hospital. It started on people’s wrists.
Early wearables—the first-generation fitness trackers of the early 2000s—tracked step counts and little else. Basic, consumer-facing, and clinically irrelevant. Fast forward two decades, and the landscape looks fundamentally different. According to a Health Information National Trends Survey, one in every three Americans now uses a wearable device to track their health and fitness.
More importantly, the devices themselves have transformed. Today’s medical-grade monitors—continuous glucose monitors (CGMs), wearable ECG patches, biosensors, smart patches for medication delivery—are FDA-cleared, clinically validated, and capable of generating continuous physiological data streams that rival what was previously possible only in a hospital room.
Consider the breadth of what’s now available. Devices like the VitalPatch® (VitalConnect), BioButton® (BioIntelliSense), and Radius VSM® (Masimo) are FDA 510(k)-cleared and CE-marked, deployed across perioperative, post-ICU, general ward, and long-term home monitoring contexts. The CardioWatch 287-2® and SensiumVitals® are seeing use in emergency transport and continuous surveillance settings. These aren’t fitness accessories—they’re clinical instruments with validated accuracy and real-world deployment in high-acuity environments.
Patient-generated health data (PGHD) has moved from an interesting concept to a core component of chronic disease management. Wearables now monitor hypertension, diabetes, COPD, and cardiac conditions continuously—alerting care teams to deviations before they escalate. The global remote patient monitoring market reflects this shift. Valued at $5.2 billion, it’s projected to grow at a compound annual growth rate of 18.6% through 2030 (Grand View Research).
For healthcare institutions, that growth trajectory represents both a clinical opportunity and a financial one—provided billing infrastructure keeps pace with clinical adoption.
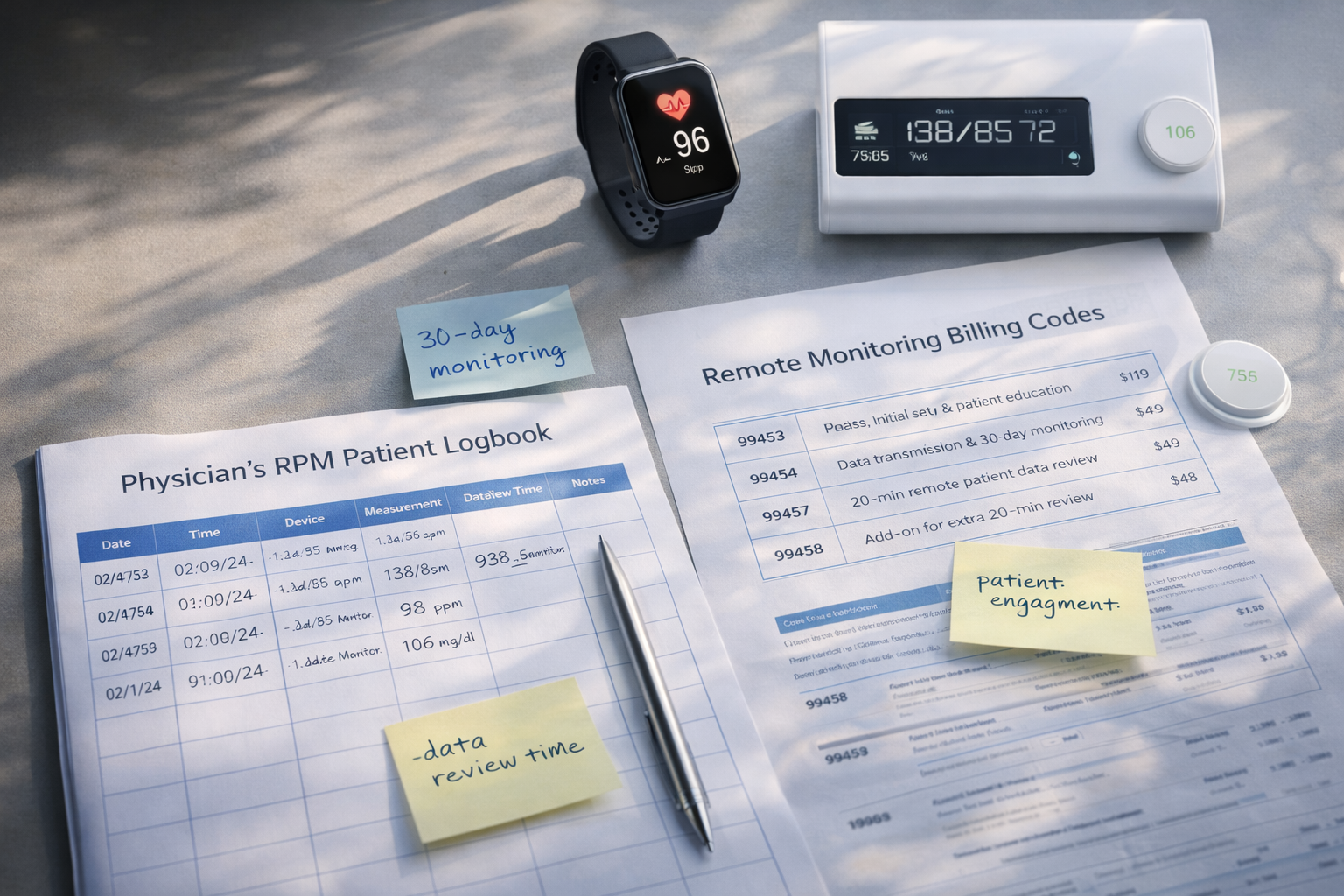
Strategic Billing Opportunities: CPT Codes 99453, 99454, and 99457
The CMS has responded to the rise of RPM with a dedicated reimbursement framework. Three CPT codes sit at the center of it.
CPT 99453 — Initial Setup and Patient Education
This code covers the remote monitoring of physiologic parameters—weight, blood pressure, pulse oximetry, respiratory flow rate—with a specific focus on the initial setup of equipment and patient education. It’s a one-time billing event per patient, but it’s foundational. Without proper documentation at setup, downstream billing becomes vulnerable to denial.
CPT 99454 — Device Supply with Daily Recordings or Programmed Alerts
Billed per 30-day period, CPT 99454 covers the ongoing supply of the monitoring device, along with daily recordings or programmed alert transmissions. A critical compliance requirement: the patient must use the device for at least 16 days within the billing period. This is one of the most common failure points for RPM programs. Organizations without automated tracking frequently bill for periods where device usage falls short of the threshold—a predictable source of denials and recoupment risk.
CPT 99457 — Treatment Management Services
This code covers 20 or more minutes of clinical staff, physician, or other qualified healthcare professional time in a calendar month, with a requirement for interactive communication with the patient or caregiver. An add-on code, CPT 99458, can be billed for each additional 20-minute increment.
Together, these codes create a recurring monthly reimbursement model for chronic care patients enrolled in RPM programs. For a practice managing a patient panel of several hundred RPM-enrolled patients, the revenue potential is substantial. The operational challenge—and the key to financial sustainability—is ensuring that documentation, device compliance, and clinical time tracking hold up against CMS scrutiny.
Read More: Protect Your Practice: A Complete Guide to Ethical Billing, Upcoding Risks And Reducing Downcoding
Enhancing Reimbursement with FinanceCore AI
The bottleneck in most RPM billing programs isn’t clinical intent. It’s data accuracy and workflow consistency.
FinanceCore AI addresses this by automating the data validation processes that are most prone to human error. Rather than relying on staff to manually reconcile device usage logs, monitor billing thresholds, or flag incomplete documentation, FinanceCore AI integrates with RPM platforms and EHR systems to provide real-time compliance tracking against CMS requirements.
Practically, this means:
- Automatic threshold monitoring: FinanceCore AI tracks device usage days against the 16-day requirement for CPT 99454, triggering alerts before a billing period closes with insufficient data.
- Documentation completeness checks: Before a claim is submitted, the system verifies that all required elements—patient consent, setup documentation, time logs for CPT 99457—are present and compliant.
- Coding accuracy: AI-driven coding tools reduce undercoding and overcoding errors, ensuring reimbursement is maximized within the bounds of what’s clinically supported.
- Payer-specific rule engines: CMS guidelines don’t apply uniformly across all payers. FinanceCore AI applies payer-specific logic to reduce the friction that comes from billing RPM services to commercial insurers with differing requirements.
The downstream effect of better data accuracy isn’t just cleaner claims—it’s faster payment cycles and a measurable reduction in administrative overhead spent on claim corrections.
Reducing Denials: Addressing Documentation and Reporting Pitfalls
RPM-related claim denials share a short list of root causes. Identifying and systematically addressing each one is where most programs find their biggest financial gains.
Insufficient device usage documentation
As noted above, CPT 99454 requires 16 days of device use per 30-day period. If the documentation doesn’t clearly establish this, the claim is exposed. Organizations need automated reporting tools that produce an audit-ready log of usage days—not just a summary statement from the device vendor.
Failure to establish medical necessity
CMS expects clear documentation of why RPM is medically appropriate for each enrolled patient. Chronic disease diagnoses (hypertension, diabetes, CHF) provide a strong foundation, but the clinical record must explicitly support the monitoring protocol in place.
Missing interactive communication documentation
CPT 99457 requires interactive communication—a phone call, video visit, or similar exchange—not simply passive data review. A clinical note that logs a data review without documentation of patient interaction will not support the code. Staff education on this distinction is essential.
Inappropriate enrollment criteria
Not all patients qualify for RPM billing under CMS guidelines. Patients must have an established relationship with the billing provider, and certain settings and provider types carry additional restrictions. Billing RPM for ineligible patients is a common compliance risk that AI-driven eligibility screening can substantially reduce.
Coordination of care conflicts
RPM codes cannot be billed during the same service period as certain other chronic care management codes without specific attention to avoiding overlap. FinanceCore AI’s compliance engine flags these conflicts before claims are submitted, preventing denials that would otherwise require manual review and resubmission.
Read More: The Hidden Risks of AI in Healthcare: Ensuring PHI Security Amid Data Explosion
Data Integration and Security: Navigating EHR Interoperability and HIPAA
Wearable devices generate data in dozens of proprietary formats. Getting that data into an EHR system—cleanly, securely, and in a format that supports clinical decision-making—is still one of the more technically demanding aspects of running an RPM program.
Open APIs and standardized data protocols such as HL7 FHIR have significantly improved interoperability between wearable platforms and major EHR systems. The key is ensuring that the RPM platform your organization selects has native integrations with your EHR, rather than requiring manual data transfer processes that introduce latency and error risk.
On the security side, the stakes are high. There were more than 700 cyberattacks involving 500 or more patient or customer records compromised in 2021 alone. HIPAA compliance isn’t optional—it requires end-to-end encryption of data in transit and at rest, access controls limiting data visibility to authorized personnel, and regular audit trails.
The NIST Cybersecurity Framework provides a practical structure for assessing and strengthening your organization’s security posture around wearable data. Combined with HIPAA compliance certification and ISO 27001 standards, it establishes a defensible foundation for programs that are managing continuous data streams from thousands of patients.
Edge computing and cloud computing models both have roles to play. Edge computing enables data processing directly on the device or a local gateway—useful in environments with limited connectivity. Cloud computing supports centralized analysis and real-time dashboard access for clinical teams. Many enterprise RPM programs use a hybrid of both, ensuring continuity even when internet connectivity is interrupted.
Predictive Analytics in Risk Management: From Reactive to Proactive Care
The clinical case for RPM is, at its core, a case for earlier intervention.
Traditional monitoring operates on a reactive model—vital signs checked at scheduled intervals, interventions triggered after symptoms appear. This approach leaves what researchers describe as a “care blind spot”: the period between scheduled checks when patient status can change significantly without clinical awareness.
Wearable devices with AI-driven analytics close that gap. Continuous trend analysis detects physiological deterioration before it becomes clinically apparent—not by tracking absolute values, but by identifying deviations from each patient’s individual baseline. This personalized approach is far more sensitive than population-level thresholds.
The clinical data supporting this shift is compelling. Wearable devices combined with predictive algorithms have demonstrated the ability to anticipate critical events up to 14 to 15 hours before clinical manifestation. An advanced wearable AI system for sepsis prediction (SepAl) has shown the capacity to predict sepsis onset up to 9.8 hours in advance using PPG sensors, temperature measurement, and accelerometer data.
For chronic disease management programs specifically, wearable technology has shown the potential to reduce hospitalizations by as much as 30%. Remote patient monitoring could eliminate up to 63% of emergency room visits. These figures represent both better patient outcomes and lower total cost of care—a direct financial benefit for organizations operating under value-based care models.
Predictive analytics also supports smarter staff deployment. Rather than triaging all patients at the same scheduled intervals, clinical teams can prioritize attention toward patients whose data indicates emerging risk. This is operationally significant in settings with constrained staffing, which describes most healthcare organizations today.
Future-Proofing Financial and Clinical Operations Through Integrated Remote Monitoring
Remote Patient Monitoring (RPM) is no longer an emerging opportunity—it is a rapidly expanding reimbursement channel. CMS continues to refine its coding framework for remote monitoring, and commercial payers are following closely behind. The signal is clear: healthcare organizations that build strong RPM infrastructure today will capture significant financial and clinical advantages tomorrow. At Care Medicus, we see RPM not just as a clinical innovation, but as a strategic revenue opportunity for organizations prepared to operationalize it correctly.
Success in RPM requires more than distributing wearable devices. It demands platforms that automate compliance tracking, standardized documentation workflows that support accurate billing, and audit-ready reporting that ensures clean claims submission. It also requires selecting clinically validated wearable devices with clear FDA clearance and seamless EHR integration, while training both clinical and administrative teams to understand the protocols and billing rules governing RPM programs.
The opportunity is not theoretical—it is already embedded in CMS fee schedules. The organizations capturing that value are those with the operational discipline to document accurately, monitor device usage consistently, and verify interactive communication requirements before claims are submitted.
Start by auditing your current RPM documentation workflows. Identify where device usage tracking breaks down, where communication requirements are missed, and where claims move forward without full compliance verification. These gaps represent immediate opportunities for improvement—and for revenue recovery. Tools like FinanceCore AI help transform documentation vulnerabilities into intelligent compliance checks, ensuring RPM claims are submitted correctly the first time.
With deep expertise in RPM program optimization and AI-driven revenue cycle intelligence, Care Medicus helps healthcare organizations align clinical innovation with billing precision. Wearables and remote monitoring are already reshaping patient care—the organizations that pair those clinical capabilities with disciplined billing infrastructure will be the ones that scale successfully into the next decade.
Leave a Reply